
What is Amalgam tattoo?
Amalgam tattoo are bluish-grey or black macules observed on clinical examination in oral mucosa, attached gingiva and other oral tissues adjacent to the amalgam-restored teeth and roots.
Amalgam tattoo is an exogenous foreign toxic amalgam material implanted in to the alveolar soft and hard tissue by your dentist or oral surgeon.
The histopathological feature of amalgam tattoos is normally the presence of impregnated small and dark granulated amalgam particles into soft tissues of the oral cavity.
As opposed to the An X-ray mucosal melanoma, dispersed amalgam particles are viewed as shiny radiopaque fragments in the radiographs, To exactly locate the amalgam particles 3-dimensional radiographs type CBCT is required, prior to the surgical removal planning.
What are the causes of amalgam tattoo?
- – Iatrogenic implantation during extraction of crushed and fractured heavily amalgam-restored teeth. To avoid undue amalgam deposition, ingestion or impregnation, in particular in the fractured teeth, your dentist should carefully remove every amalgam particles under SMART protocol (Case report 1.).
- Endodontic retrograde root apex obturation following root apicectomy procedure (Case report 2.).
What is the biological treatment of Amalgam tattoos?
Conservative surgical excision of amalgam fragments is indicated when there are issues of aesthetic or adverse biological health concerns.
Case report 1:
A 35-year-old woman presented with black macule around the buccal and palatal gingival margins of the tooth upper left four. She reported the emergence of amalgam tattoo as a result of non-biological tooth extraction causing crushing and implantation of the amalgam fragments into socket of her milky tooth at the pre-adolescent age.
Clinical presentation: The Amalgam tattoo extended and impregnated to the palatal cortical bone along the marginal buccal cortex in the axial direction formed cavitation.



Intraoral images at the time of clinical examination

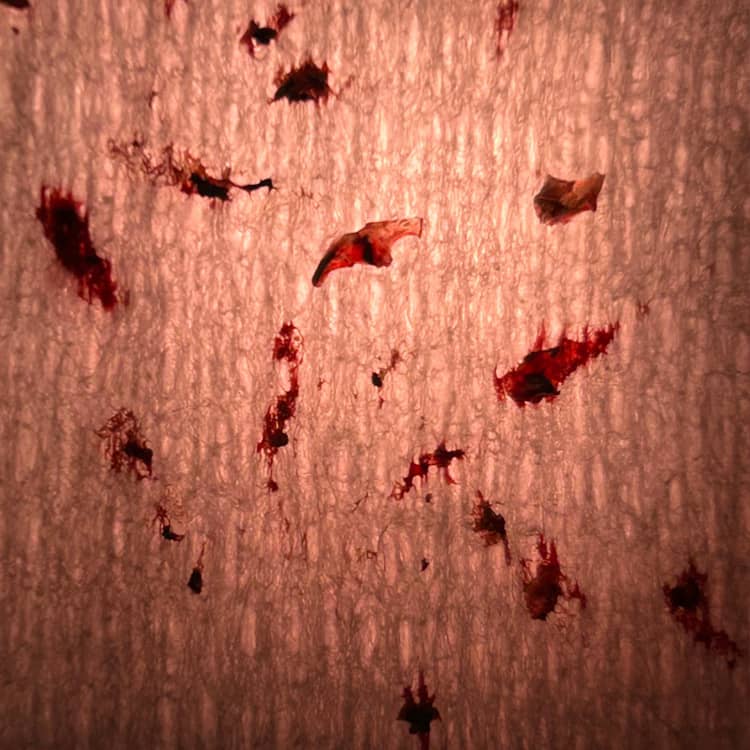
Images of the surgically explanted amalgam particles
Wat is the treatment of amalgam tattoo?
The Amalgam tattoo was removed with a round diamond Piezo and current hand instruments. Clinical photos were taken. A laterally-positioned pedicle flap covered the exposed surgical region.
Case report 2:
A 55-year-old lady presented with Heavy metal contamination; she has been working with a Functional Medicine Therapist to try to understand why I keep getting sick. Both blood and urine tests show high levels of toxic elements, e.g. mercury and arsenic. She suffered from chronic hyperparathyroidism and had 2 parathyroid glands removed. She had breast cancer and mastectomy. She received radiotherapy for her non-Hodgkin’s Lymphoma. She referred to us to treat her unresolved residual infection around the roots of teeth lower right one (LR1) and left one (LL1).
Toxicology blood test:
She presented with the history of car accident at the age of 8, when she smashed and traumatised her lower front teeth. She received root canal treatment and crowns following teeth pulp necrosis.
Her toxicology blood test revealed high blood-born Cadmium, Arsenic, and Mercury titres despite her healthy diet and lifestyle. She suggested this could be due to the chronic slow release of the heavy metal traces released to her blood circulation after retrograde apical amalgam plugs inserted during the apicectomy procedures at the age of 8.
As a result of unsuccessful root canal treatment and recurrent abscesses her lower front teeth had to be treated implementing apicectomy and retrograde root-plugging using amalgam at the age of 10.
Tooth LR1 presented with incomplete root canal obturation; apicectomy with retrograde amalgam plug, limited chronic periapical radiolucency and Guarded prognosis.
Periapical pathology LL1:
The LL1 has a single root canal, but this is unfilled. However, there is retrograde amalgam at the LL1 from previous apical surgery. A 3.5 mm area of periapical radiolucency persists at the LL1.

Preoperative views
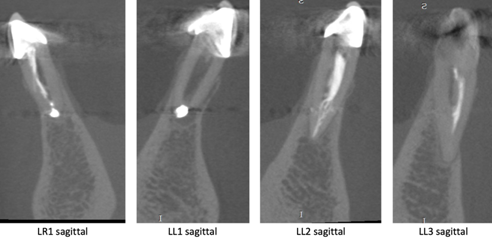
Image Cone Beam CT
Wat is the treatment of amalgam implantation?
Revision of the RCT was performed using an initial non-setting antibacterial agent followed by definitive RCT and crown. At the next appointment the tips of the roots were surgically approached to remove the amalgam plugs safely. The surgical bone defects were regenerated using the bone augmentation technique.