

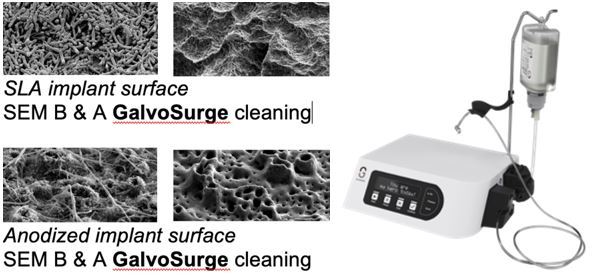
GalvoSurge: Electrolytic Implant Surfaces Cleaning
The unique GalvoSurge mode of action completely decontaminates the biofilm from any inaccessible contaminated titanium implant surface bio-compatible for complete bone-fill & re-osseointegration. Significant radiographic bone gain, reductions in PPD, BoP, and suppuration is achieved and maintained over an 18-mon. period (Schlee et al. 2021).
Implant Complications
Osseointegration is a process by which a clinically asymptomatic rigid direct fixation between an implant and surrounding living bone is achieved and maintained under functional loading (Zarb & Albrektsson 1991). One of the key factors in the long-term success of dental implants is maintaining healthy tissues around them. Bio-mechanical complications include the failures of the hardware components, e.g. fracture of the implants, coatings, connecting screws and prostheses. Biological complications may lead to primary early failures by interfering with the process of osseointegration or secondary late failures to maintain the achieved osseointegration.
Bio-mechanical Complications
Experimental evidence indicates that early biomechanical overloading in excess of a critical micro-motion of 100µ (Brunski 1999) may disturb an early bone apposition during the bone remodelling phase and divert the process of osseointegration to an early reversible implant fibro-integration (Szmukler-Moncler et al. 2000).
Iatrogenic failures may be caused by the mal-positioning of implants, rendering the restoration of the implant impossible due to functional, technical and aesthetical complications or may be caused by violation of the anatomical structure, requiring implant explantation (Esposito et al. 1998).
Excessive surgical trauma and premature loading (iatrogenic factors) together with impaired healing ability, infection and insufficient bone volume and quality (host-related factors) are believed to be responsible for the early (47%) implant failures, while biomechanical overloading (90%), and progressive chronic marginal infection presenting as peri-implantitis (10%) are shown to have the predominant role in the late (53%) implant failures (Esposito et al. 1998).
Insufficient bone quantity and quality compromising para-implant biomechanical capability, coupled with supra-physiological implant functional overloading exceeding 4000 me during the process of late-bone –remodelling, has been associated with implant fibrous encapsulation and late biomechanical failures (Lanyon et al. 1975). Furthermore, implant aseptic loosening is caused by supra-physiological bone strain ≥ 6,000 μέ during the implant’s late functional loading (Meyer et al. 2001).
Prevention & Treatment of implant Bio-mechanical Complications
Excessive loading, unfavourable number, distribution, surface, characteristics and design of the supporting implants are associated with biological failures of oral implants. To prevent or undertake remedial treatment to address the implant bio-mechanical complication, the following strategies should be considered:
- Increasing the number of supporting implants
- Optimise the mechanical equilibrium and distribution of occlusal loadings
- Optimise the loading vectors and reduce the collision of the occluding surfaces
- Increasing the diameter of implant-abutment interface dimensions
- Enhancing the mechanical properties of the abutment retaining screws
- Improving the porcelain/acrylic/metal bonding strength.
- An early detection of failures and remedial intervention is recommended during the treatment reviews and maintenance sessions.
Biological Complications
The body of evidence from the recent literature suggests that poor oral hygiene, history of periodontitis, uncontrolled diabetes and heavy smoking, compromised host tissues or immune response, poor bone quality, bone grafting, irradiation therapy, parafunctional activities, the degree of surgical trauma, bacterial contamination, compromised host tissues or immune response to be associated with biological failures of oral implants.
Biological risk factors
Biological risk factors contributing to implant failures can be divided into endogenous (systemic and local) and exogenous (operator-related & biomaterial-related) risk factors.
Endogenous systemic risk factors include age & genetics, medical status of the patient, and smoking.
Endogenous local risk factors include bone quality, quantity and anatomical location, bone grafting, parafunction & biomechanical loading, local immune response, presence of “adequate” attached keratinised soft tissue, and irradiation therapy (Esposito et al. 1998).
Despite changes in mineral composition, clinical investigations seem to reject the assumption of the adverse role of age in implant success (Jemt 1993). At present, there exists inadequate information on the importance of genetic factors on implant survival.
The following nutritional status, general diseases and disorders have been suggested to adversely affect the outcome of the implant treatment: uncontrolled bone metabolic disease (e.g. osteoporosis, osteomalacia, hyperparathyroidism & Paget’s disease); advanced rheumatic diseases (e.g. rheumatoid arthritis, Sjogren’s disease, systemic lupus erythematosus); uncontrolled hormonal disease (e.g. diabetes, Cushing’s syndrome, hyperparathyroidism); lichen Planus, PMN anomalies, delayed hypersensitivity & immunological disorders; and malabsorption syndrome.
Peri-implant disease is a collective term for inflammatory reactions in the surrounding tissue of the functioning implant. Peri-implant mucositis is a term describing reversible inflammatory reactions in the surrounding soft tissue of a functioning implant.
Prevention & Treatment of implant Biological Complications
- Peri-implant Recession
- Peri-implant Mucositis
- Peri-implantitis
- Failing implants
1. Peri-implant Recession
Similar to periodontal mucogingival deficiencies (MGD), peri-implant mucogingival deficiencies (PIMGD) is a sequel of inadvertent gum recession around the osseointegrated dental implants. The apical migration of the peri-implant soft tissue margin as a result of a variety of factors may cause aesthetic disturbance, exposure of the implant abutment and in advanced cases, the implant head exposure.
Etiologic factors associated with peri-implant mucogingival deficiencies:
- Buccal implant positioning
- Inadequate buccal soft tissue thickness
- Excessive implant-head proclamation
- Incompatible to restorative compensation
- Inadequate or excessive implant-implant or implant-tooth interproximal space
- Disintegration of the buccal bone grafting material
- Collapse of the non-rigid GBR membrane
- Postoperative soft-tissue graft complications
An ideal soft tissue thickness of ≥ 2mm with a height of 3-4 mm is required to protect the implant, abutment and the margin of the restoration. Classification of the PIMGD has been made on similar biological principles in terms of extent and severity applied to periodontal MGD. Hence, similar guidelines may apply to the regeneration of PIMGD.
The prognosis for the soft tissue augmentation is determined by the extent and severity of the defect and the implant abutment dimension, position and angulation.
2. Peri-implant Mucositis
Peri-implant mucositis refers to inflammatory reactions around functioning dental implants leading to marginal soft tissue redness, bleeding and increased peri-implant pocket depth (PIPD). The implementation of non-surgical mechanical and adjunctive use of local/systemic antimicrobial therapy to reduce the peri-implant inflammation has been proven to be effective for the resolution of peri-implant mucositis lesions but unpredictable for the effective treatment of advanced peri-implantitis lesions.
3. Peri-implantitis
Peri-implantitis refers to inflammatory reactions around functioning dental implants leading to the loss of supporting bone (Albrektsson & Isidor 1994). Peri-implantitis has been defined as a progressive inflammatory bacterial-infectious process deteriorating and destructing the supporting soft and hard tissues around functional osseointegrated implant, eliciting bacterial, clinical and radiographic signs and symptoms, e.g. bleeding and suppuration (Mombelli et al. 1987).
The existing scientific evidence demonstrates a direct association between the accumulation of oral microbiota and the development of inflammatory lesions in the form of Peri-implant mucositis or peri-implantitis (Pontoriero 1994).
In both experimental research and human trials (Lang et al. 2000), it has been shown that prolonged bacterial accumulation over a long period of time may convert the reversible nature of peri-implant mucositis into irreversible peri-implantitis. As a result, the disease of peri-implant mucositis (ailing) amenable to treatment may become untreatable (failing).
Diagnosis of Peri-implantitis
To monitor the peri-implant health status, following the insertion of definitive restoration, baseline standardised radiographs and peri-implant probing depth (PIPDs) should be recorded as references for the comparison to the future radiographs and PIPDs chart.
Following the initial bone remodelling, the presence of radiographic evidence of marginal bone loss (MBL) coupled with the clinical presence of inflammation, e.g., bleeding on probing (BOP), suppuration, and increased PIPDs may reflect the extent and severity of existing pathological status, and the diagnosis of peri-implant disease.
Treatment of Peri-implantitis
The existing published literature on Peri-implantitis yet fail to provide evidence for sufficient effectiveness of advocated strategies implemented in the treatment of peri-implantitis. Based on the accumulated data from both experimental research and clinical trials, these treatment categories are classified into 2 categories:
Nonsurgical therapeutic strategies
The aims and objectives of the nonsurgical peri-implant treatment strategies are to:
- Eliminate the peri-implant granulation tissues;
- Decontaminate the implant surface (e.g. laser devices, adjunctive local sustained delivery antimicrobial agents /systemic antibiotics alone or in combination).
- Debride the peri-implant biofilm utilizing mechanical surface debridement (e.g. carbon or plastic curettes, ultrasonic, and air abrasive devices);
The review of the literature on the various nonsurgical treatment strategies for peri-implant lesions in both experimental research and human studies provides evidence that most of the nonsurgical treatment modalities aiming to reduce the submucosal infection, may result in a short-term improvement of peri-implantitis.
Surgical therapeutic strategies
The aims and objectives of surgical peri-implant therapeutic strategies are to:
- Eliminate the peri-implant granulation tissues
- Eradicate the interfacial biofilm by employing mechanical surface debridement (e.g. ultrasonic, carbon curettes, air abrasive)
- Decontaminate the infected interface via non-mechanical surface decontamination techniques (e.g. laser devices, adjunctive local sustained-delivery antimicrobial agents, systemic antibiotics).
- Modify the implant surface macro-architecture to eliminate the surface retention niche for pathogens employing implantoplasty.
- Bio-surface modification to promote re-osseointegration (L-PRF)
- Restoration/ regenerative of the peri-implant lesions
- Novice GalvoSurge: achieves complete surface cleaning followed by full or significant bone fill ready for re-osseointegration (schlee et al. 2019). Electrolytic cleaning does not harm soft and hard tissues
The extent and quality of bone regeneration and osseo-reintegration/ BIC (bone-implant contact) at the interface following the regenerative treatment of peri-implantitis lesions have been variable in various trials and case reports. This could be because the currently advocated regenerative techniques are not performed consistently based on the specific indication criteria. Therefore, due to an inappropriate clinical protocol, insufficient debridement and elimination of the residual debris may have not resulted in efficient interface decontamination.
The current treatment modalities advocated in the treatment of peri-implantitis have been reported to exert some beneficial and successful effect. However, up to the present, none of these therapeutic strategies has proved to be the most efficacious when treating advanced peri-implantitis. Incomplete debridement and surface decontamination or disinfection seem to be the major obstacle in resolving the peri-implant lesion, bone regeneration and osseo-reintegration.
These findings consistently indicate that up to the present, there is no specific individual or combination treatment strategy that has yet been recognised as a gold standard approach for the treatment of peri-implantitis, and that the currently available evidence does not verify the superiority of each specific technique in certain sub-type of peri-implantitis. Therefore, the diagnostic procedure and interceptive treatment of destructive peri-implantitis should be attempted at the earliest stage of disease progression.
Failing implants with advanced peri-implantitis
Implants with advanced extent of peri-implant osseo-disintegration when presenting with radiographic marginal bone loss exceeding 60% and/or clinical PIPD of 10mm, bleeding or pus exudate on probing are explanted. The residual defect is then treated using guided bone regenerative techniques. After ca. 6 months of healing, a new implant may be placed.
PATIENT REFERRALS
We welcome referrals from our referring colleagues to undertake specialist multi-disciplinary procedures as below:
- Treatment of implant biomechanical failures
- Treatment of peri-implant mucositis by EMS Perio. Glycine powder
- Treatment of peri-implantitis using the novel NB Galvosurge™ electrolyte surface-cleaning.
- Non-invasive implant Explantation and guided Bone Regeneration.
- In order to improve and secure long-term clinical success, we strongly advise that all the referred patients pursue Postoperative Individualised Supportive Periodontal or Supportive Peri-implant Treatment (SPT).