
Last Updated on June 25, 2025 by Dr. Nico Kamosi
How do we diagnose Peri-implantitis?
Following the insertion of definitive restoration, baseline standardized radiographs and peri-implant probing depth (PIPDs) should be recorded as references for comparison to the future radiographs and PIPDs chart to monitor the peri-implant health status.
Following the initial bone remodelling, radiographic evidence of marginal bone loss (MBL) coupled with the clinical presence of inflammation, e.g., bleeding on probing (BOP), suppuration, and increased PIPDs, may reflect the extent and severity of existing pathological status and the diagnosis of peri-implant disease.
How do we Treat Peri-implantitis?
The existing published literature on Peri-implantitis fails to provide evidence for sufficient effectiveness of advocated strategies implemented in treating peri-implantitis. Based on the accumulated data from both experimental research and clinical trials, these treatment categories are classified into two categories:
- Nonsurgical therapeutic strategiesThe aims and objectives of the nonsurgical peri-implant treatment strategies are to:
- eliminate the peri-implant granulation tissues;
- decontaminate the implant surface (e.g. laser devices, adjunctive local sustained delivery antimicrobial agents /systemic antibiotics alone or in combination).
- debride the peri-implant biofilm utilizing mechanical surface debridement (e.g. carbon or plastic curettes, ultrasonic, and air abrasive devices);
The literature review on the various nonsurgical treatment strategies for peri-implant lesions in both experimental research and human studies provides evidence that most nonsurgical treatment modalities aiming to reduce submucosal infection may result in a short-term improvement of peri-implantitis.
- Surgical therapeutic strategies:The aims and objectives of surgical peri-implant therapeutic strategies are to:
- eliminate the peri-implant granulation tissues
- eradicate the interfacial biofilm by employing mechanical surface debridement (e.g. ultrasonic, carbon curettes, air abrasive)
- decontaminate the infected interface via non-mechanical surface decontamination techniques (e.g. laser devices, adjunctive local sustained-delivery antimicrobial agents, systemic antibiotics).
- modify the implant surface macro-architecture to eliminate the surface retention niche for pathogens employing implantoplasty.
- Bio-surface modification to promote re-osseointegration (L-PRF)
- Restoration/ regenerative of the peri-implant lesions
- Novice GalvoSurge: achieves complete surface cleaning followed by full or significant bone fill ready for re-osseointegration (schlee et al. 2019). Electrolytic cleaning does not harm soft and hard tissues
The extent and quality of bone regeneration and osseo-reintegration/ BIC (bone-implant contact) at the interface following the regenerative treatment of peri-implantitis lesions have been variable in various trials and case reports. This could be because the currently advocated regenerative techniques are not performed consistently based on the specific indication criteria. Therefore, due to an inappropriate clinical protocol, insufficient debridement and elimination of the residual debris may have not resulted in efficient interface decontamination.
The current treatment modalities advocated in the treatment of peri- implantitis have been reported to exert some beneficial and successful effect. However, up to the present, these therapeutic strategies have yet to prove to be the most efficacious when treating advanced peri- implantitis. Incomplete debridement and surface decontamination or disinfection seem to be the major obstacle in resolving the peri-implant lesion, bone regeneration and osseo-reintegration.
Conclusion
These findings consistently indicate that up to the present, there is no specific individual or combination treatment strategy that has yet been recognised as a gold standard approach for the treatment of peri- implantitis, and that the currently available evidence does not verify the superiority of each specific technique in certain sub-type of peri- implantitis. Therefore, the diagnostic procedure and interceptive treatment of destructive peri-implantitis should be attempted at the earliest stage of disease progression.
GalvoSurge: Electrolytic Implant Surfaces Cleaning
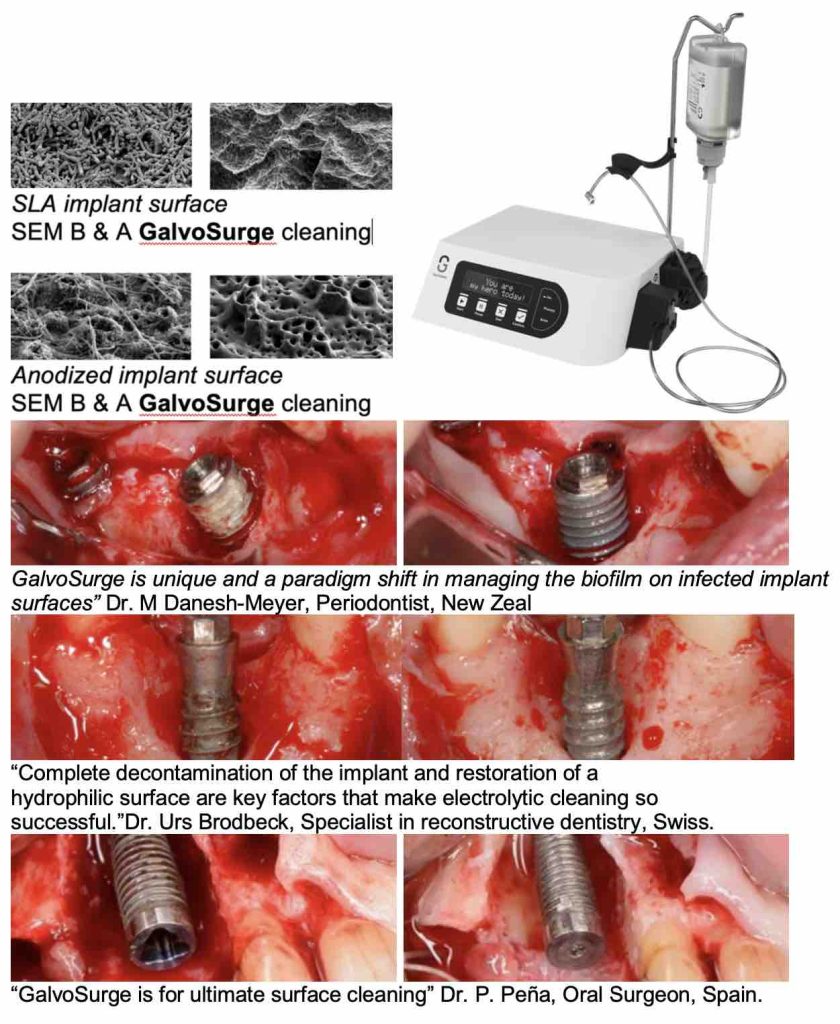
The unique GalvoSurge mode of action completely decontaminates the biofilm from any inaccessible contaminated titanium implant surface bio- compatible for complete bone-fill & re-osseointegration. Significant radiographic bone gain, reductions in PPD, BoP, and suppuration is achieved and maintained over an 18-mon. period (Schlee et al. 2021).
GalvoSurge is unique and a paradigm shift in managing the biofilm on infected implant surfaces.
”Dr. Urs Brodbeck, Specialist in reconstructive dentistry, Swiss.
“GalvoSurge is for ultimate surface cleaning” Dr. P. Pena, Oral Surgeon, Spain.
” Dr. M Danesh-Meyer, Periodontist, New Zeal
“Complete decontamination of the dental implant and restoration of a hydrophilic surface are key factors that make electrolytic cleaning so successful.
PATIENT REFERRALS
We welcome referrals from our referring colleagues to undertake specialist multi-disciplinary procedures as below:
- Treatment of implant bio-mechanical failures
- Treatment of peri-implant mucositis by EMS Perio. Glycine powder
- Treatment of peri-implantitis; using the novel NB GalvosurgeTM electrolyte surface-cleaning.
- Non-invasive implant Explantation & Guided Bone Regeneration.
- In order to improve and secure a long-term clinical success, we trongly advise that all the referred patients pursue Postoperative Individualised Supportive Periodontal, or Supportive Peri-implant Treatment (SPT).
Dr Nico Kamosi is a GDC registered Specialist in Periodontics. He has been teaching the science and clinical application of Periodontology and Implantology to both undergraduates and postgraduates for more than 10 years. He was a Reviewer of Journal of Oral and Maxillofacial Implants (JOMI). One of his main special interest is treatment of implant Bio-mechanical complication.

Dr. Nico Kamosi
Dr. Nico Kamosi
Specialist Periodontist, Implantologist, Prosthodontist, Holistic and Biological Dentist
TDL. DDS. (Swe.), MSc.Perio.(Eng.),
MClinDent.Perio.(Eng.), MSc.Imp.Dent.(Eng.),
Dip.Aesth.Med. (Eng.), MClinDent.Prosth.(Eng.),
Cert., Dip.DHSLM.(RCS.Eng.), Cert.Orth.(Eng.), Cert.Law (Eng.), AIAOMT
Accredited member of IAOMT, SMART Certified
Member of AACD, EFP, AAP, ESCI, IAOMT