
Could infected root canal treated teeth elicit autoimmune diseases and other health hazards?
Progression of the unresolved reinfected root canal – A case report
A young lady presented with concerns about the progression of the unresolved reinfected root canal-treated upper central incisor and bone loss. She expressed her concern about the immunological and biological impact of intermittent infection elicited from the reinfected root canal-treated upper central incisors. Therefore, she requested biological extraction of the tooth upper right one (UR1) and possible retrograde removal of the foreign element remnant following a second root canal treatment (RCT) of tooth upper left one (UL1).
She explained that tooth UR1 has been retreated 3 times; hence requested biological extraction of this tooth followed by a provisional resin-bonded zirconia bridge and later a permanent single crown supported on a Zirconia dental implant.
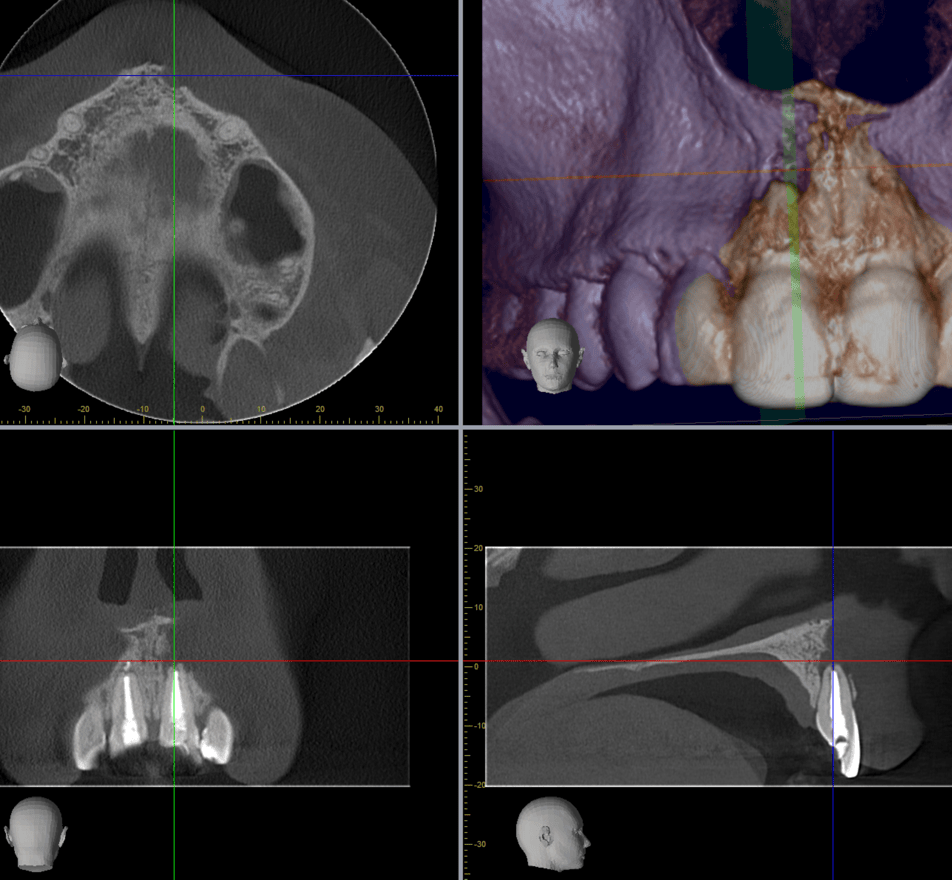
The CBCT radiographic investigation revealed apical periodontal infection and extensive bone loss around the tooth UR1 and foreign element remnant (Guttapercha) at the tip of the root UL1. Tenderness on vestibular pressure (palpation); extensive apical fenestration through the buccal bone plate; Peri-apical widened PDL, bone resorption, and interrupted lamina dura rendered prognosis of the tooth UR1 very poor.
Patient was informed about the procedures involved in the biological atraumatic extraction involving: 1) Mechanical debridement of granulation tissues and periodontal ligament using special instrument; removal of the infected bone 2) Chemical debridement and disinfection using Ozonated saline 3) L-PRF to enhance the tissue healing 4) Bone augmentation 5) biomodulation for accelerated healing.
Following the biological extraction an interim fixed-hybrid Maryland dental-supported Zirconia bridge was used to replace the tooth UR1 while waiting for the bone augmenting materials to be integrated.
The patient was advised that she could be referred to a specialist endodontist for a 2nd opinion to undertake revision of her root canal treatment. However, she stated that she already has undertaken RCT revision of the tooth UR1 and UL1; the patient requested the removal of the tooth UR1 as she was convinced that her health has been compromised since the RCT failures and reinfected root canal treatments.
Following atraumatic biological extraction of tooth UR1 and removal of foreign body at the tooth UL1, a satisfactory post-operative healing was achieved and the mild PO-swelling and discomfort was abating unevenly. Patient was advised that six months of healing time is required before a late-staged Zirconia dental implant placement could be performed.
Clinical relevance:
Factors such as genetic, environmental, the number of root canal teeth, pre-existing pulp conditions, patient’s immunological health status may determine if a root canal tooth pose any specific systemic health risk for the patient.
Therefore, it is crucial to undertake proper clinical and radiographic evaluations before developing a comprehensive individualised treatment plan to address any oral health concern that may interfere with the individual’s general health.
Immunological health problems such as muscular skeletal disease, fibromyalgia, and inflammatory bowel disease have been associated with infected root canal treated teeth.
Dentin microtubule could be an ideal space for accumulation and growth of most harmful anaerobic bacteria which produce metabolic by-products that may enter the blood circulation. The difference and complexity in the number and anatomy of the root canals, the undetectable presence of accessory canals and the presence of surrounding dentin layer containing about 3 miles of microscopic microtubules may render the most comprehensive treatment compromised to eliminate the source of bacterial infection from all of the microtubules, and complex root canal system.
There are a good number of case publications and internal report from the studies of patients at the cancer clinics which indicate the refer a high number of root canal infection in cancer patients. Research by Doctor Boyd Haley, a clinical toxicologist expert showed that 90 percentage of the root canals were harbored with dozens of different pathogens.
To avoid any unnecessary treatment which might compromise the patient general health, and mental well-being we should take the most conservative approach based on each patient’s individual case presentation.
There are few books published about the concerns of root canal treated teeth: “Root canal cover up” by Dr Meinig; “Death by root canal” by biological dentist Doctor. Ron Carlson; and “Let the truth be known” by. Doctor Down Ewing, a previous executive director of the International Academy of Biological Dentistry and Medicine.
Clinical considerations that determine the justification of the removal of infected root canal treated teeth:
Persistent Infection: In case of persistent infection, pain, discomfort, swelling, or the presence of a sinus tract, or if the root canal treatment is unsuccessful, extraction of the infected tooth is indicated.
Periapical Lesions: When, despite the revision of the root canal treatment, the periapical lesions are not resolved and their ongoing chronic inflammation and potential bone loss are not quickly addressed, the extraction of the tooth is indicated.
Structural Integrity: Extensive structural damage to the tooth and the root may render the restoration of the tooth compromised. Therefore, in the presence of significant loss of structure, it is difficult to restore a tooth when the roots are not salvageable through treatment or if they have been damaged during the course of endodontic treatment, i.e., perforation, zipping, fracture.
Adverse Systemic Health Concerns: The presence of persistent and chronic dental and oral infection may significantly pose a high risk to overall health, especially in people with compromised immune systems. Extraction of the tooth may be necessary to avoid immunological consequences.
Failed Root Canal Retreatment: Some posterior teeth may have complex anatomy, which renders the successful endodontic treatment compromised, causing persistent treatment failure and persistent periapical infection. A careful case, risk, time, and benefit consideration should be made when the treatment may not obtain long-term success.
Ongoing Bone Loss: when despite comprehensive treatment, there ongoing marginal and apical bone loss persists, with subclinical signs of infection or inflammation, it is to the benefit of the patient to extract the tooth and avoid further bone loss. This is especially relevant if an implant is to be placed to support future restoration. Patients’ personal preferences, desires, and expectations for the future procedure are required to be taken into consideration.
Conclusion: The option for extraction of the root canal treated tooth should be determined based on mutual agreement between the operator and patient after comprehensive clinical and radiographic assessment. The patient’s overall health and potential risks, in the short or long term, to preserve versus extracting the tooth should be considered.

Dr. Nico Kamosi
Dr. Nico Kamosi
Specialist Periodontist, Implantologist, Prosthodontist, Holistic and Biological Dentist
TDL. DDS. (Swe.), MSc.Perio.(Eng.),
MClinDent.Perio.(Eng.), MSc.Imp.Dent.(Eng.),
Dip.Aesth.Med. (Eng.), MClinDent.Prosth.(Eng.),
Cert., Dip.DHSLM.(RCS.Eng.), Cert.Orth.(Eng.), Cert.Law (Eng.), AIAOMT
Accredited member of IAOMT, SMART Certified
Member of AACD, EFP, AAP, ESCI, IAOMT