
This Africo-Carabian lady presented with the following Clinical & Radiographic Findings
Lower Left Quadrant (LLQ) – Primary area of patient’s symptoms
Apical periodontitis
The body of research has shown that apical periodontitis, also described as periapical osteitis or periapical infection, is caused by infected root canal systems. This condition has been associated with adverse systemic disease and systemic complications, with potential impacts on the cardiovascular system and an increased risk of metabolic imbalance. These effects are linked to the microbial complexity of infection within the root canal system, which contains highly resistant and resilient microbial micro-niches, or micro-ecosystems. It has not been possible to identify every bacterial flora or bacterial genus present within the root canal system. However, Enterococcus species frequently dominate and are associated with very persistent infections. Other pathogenic bacteria identified within the root canal system and periapical infections include Streptococcus and Actinomyqces species. When apical periodontitis becomes symptomatic, it appears that opportunistic pathogenic bacteria play a significant role.
Bacteremia
As a result of chronic infection caused by periapical infection or apical periodontitis, bacteria may be transmitted into the bloodstream and cause chronic or acute bacteremia. This can be associated with invasive dental procedures, as well as the condition acting as a reservoir for bacteremia, whether before or after treatment. Longitudinal studies have demonstrated that identical bacterial DNA can be detected both in the bloodstream and in infected root canal complex. This finding supports a direct pathway from oral infection to systemic circulation. In particular, Enterococcus species have been linked to cardiovascular disease and endocarditis if left untreated.
Similar to periodontitis or periodontal disease, apical periodontitis can adversely influence systemic metabolic health and disturb systemic immunologic response, regulation and balance. Even in otherwise healthy individuals, apical periodontitis, like periodontitis, has been correlated with elevated HbA1c, triglycerides, LDL cholesterol, and body mass index. These changes reflect disruption of glucose and lipid metabolism, increased insulin resistance, and tryptophan depletion, indicating an increased risk of adverse systemic impact.
The literature suggests that successful root canal treatment, has been correlated with improvement in metabolic indicators and inflammatory biomarkers. This improvement may lead to enhanced systemic health following successful root canal treatment or periapical surgery. It is therefore important to recognise the association between inflammation and metabolic inflammatory imbalance.
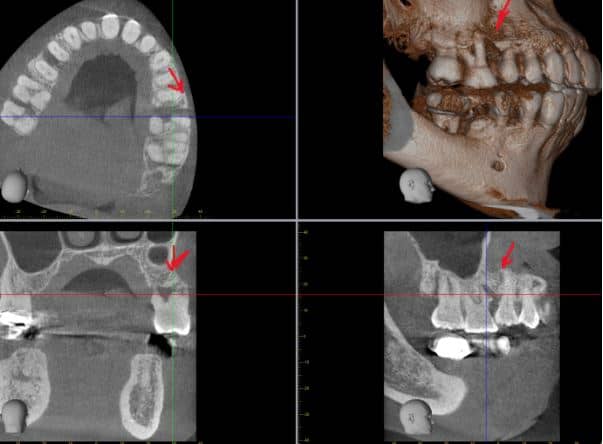
Tooth Lower Left Six (LL6): Periapical infection on both mesial and distal roots. Granulomatous changes and probable apical Cementosis with bulbous root-end formation which render the extraction challenging; requiring sectioning during extraction due to apical undercuts. The Prognosis of the tooth was deemed hopeless and surgical extraction required.
Tooth Lower Left Eight (LL8): Significant periapical infection from mesial, distal and lingual aspects. Clinical examination revealed infection tracking to the buccal soft tissues consistent with a possible draining sinus. The tooth is partially void of buccal bone plate. This tooth has a poor prognosis requiring surgical extraction with cavitation curettage required.
Both teeth demonstrate chronic apical and inter-radicular infection patterns consistent with long-standing low-grade inflammation, likely contributing to systemic inflammatory burden and immune dysregulation.
Understanding Healing Variability
Healing following biological surgery is a natural regenerative process, which varies from one individual to another. Despite meticulous care and use of advanced bioregenerative techniques, some patients may not heal smoothly or completely.
Factors influencing delayed or incomplete healing may include:
- Pre-existing chronic infections (local or systemic)
- Persistent microbial biofilm or necrotic bone residues not fully accessible during initial debridement
- Heavy metal or chemical toxicity burdens
- Impaired detoxification or liver/kidney function
- Autoimmune or inflammatory conditions
- Viral or parasitic burdens (e.g., latent herpes, Epstein-Barr, etc.)
- Nutritional deficiencies (Vitamin D, C, zinc, magnesium, collagen)
- Circulatory or lymphatic compromise
- Emotional stress or hormonal imbalance
Both surgical and systemic biological factors influence the regenerative response of the bone and soft tissues. Healing may therefore require extended time or additional biological interventions.
This case illustrates how periodontal disease is driven not only by bacteria in the mouth, but by deeper biological and metabolic processes within the body.
In this patient, advanced periodontal inflammation developed in the context of poorly controlled diabetes, hypothyroidism, cardiovascular risk factors, chronic fatigue, and reduced physical and cognitive resilience. These conditions created a biological environment in which the gums and supporting bone were unable to mount an effective healing response.
From a biological perspective, persistent hyperglycaemia alters the body’s immune and vascular systems at a cellular level. Elevated blood glucose leads to the formation of advanced glycation end products, which bind to collagen and connective tissue within the gums. This makes periodontal fibres more rigid, less elastic, and more prone to breakdown. At the same time, glycation interferes with normal collagen repair, meaning that once damage occurs, regeneration is slow and incomplete.
Hyperglycaemia also disrupts neutrophil function, impairing the first line of immune defence against periodontal bacteria. While bacterial challenge increases, the immune response becomes both weaker and more dysregulated. Pro-inflammatory cytokines such as interleukin-1β, tumour necrosis factor alpha, and interleukin-6 remain persistently elevated. This drives ongoing soft tissue inflammation and stimulates osteoclast activity, accelerating bone resorption around teeth.
Reduced microvascular circulation further compounds the problem. Diabetes causes thickening of capillary walls and reduced oxygen diffusion to periodontal tissues. As blood flow becomes compromised, delivery of nutrients, immune cells, and oxygen is reduced, while waste products and inflammatory mediators accumulate. The result is tissue that is inflamed, fragile, and poorly equipped to heal.
Hypothyroidism adds an additional metabolic burden. Thyroid hormones regulate cellular turnover, mitochondrial activity, and protein synthesis. When thyroid function is reduced, fibroblast activity slows, epithelial renewal is delayed, and bone remodelling becomes less efficient. In the oral cavity, this translates into sluggish tissue repair, increased susceptibility to infection, and delayed resolution of inflammation. Hypothyroidism is also associated with reduced salivary flow, altering the oral microbiome and allowing pathogenic bacteria to thrive.
Chronic systemic inflammation from hypertension, dyslipidaemia, and metabolic imbalance further amplifies periodontal breakdown. These conditions increase oxidative stress and endothelial dysfunction, creating a pro-inflammatory background in which local periodontal infection triggers an exaggerated destructive response. Over time, this persistent inflammatory signalling shifts the balance from tissue maintenance to tissue loss.
As periodontal inflammation progresses, inflammatory mediators enter the systemic circulation, worsening insulin resistance and perpetuating metabolic instability. This reinforces the bidirectional relationship between periodontal disease and diabetes, where each condition fuels the other in a self-sustaining pathological loop.
In this patient, physical fatigue, reduced dexterity, and cognitive decline compounded the biological vulnerability by limiting effective plaque control. This allowed bacterial biofilm to remain in prolonged contact with already compromised tissues, accelerating disease progression and reducing the effectiveness of conventional periodontal therapy alone.
For these reasons, treatment focused on removing chronic sources of infection, reducing inflammatory burden, and working alongside the medical team to stabilise systemic health. Without addressing the underlying biological drivers, periodontal stability would not be predictable or sustainable.
This case highlights a fundamental principle of holistic and biological dentistry: the mouth reflects the state of the body. Periodontal disease is not merely a local infection, but a manifestation of systemic dysregulation. Successful care requires understanding and respecting the biological cascade that links metabolism, immunity, circulation, and tissue repair.

Dr. Nico Kamosi
Dr. Nico Kamosi
Specialist Periodontist, Implantologist, Prosthodontist, Holistic and Biological Dentist
TDL. DDS. (Swe.), MSc.Perio.(Eng.),
MClinDent.Perio.(Eng.), MSc.Imp.Dent.(Eng.),
Dip.Aesth.Med. (Eng.), MClinDent.Prosth.(Eng.),
Cert., Dip.DHSLM.(RCS.Eng.), Cert.Orth.(Eng.), Cert.Law (Eng.), AIAOMT
Accredited member of IAOMT, SMART Certified
Member of AACD, EFP, AAP, ESCI, IAOMT