
What is Socket Preservation?
The extraction of the tooth as a result of tooth substance loss, fracture, infected root canals, endodontic failures, periodontal disease, trauma, et cetera, extraction is imminent and necessary. Following extraction, the bundle bone, which is an important part of the outer surface of the bone within the alveolar housing, will soon begin a resorptive process, causing bone loss mainly on the outer surface and, to some extent, on the coronal or crestal surface.
This adverse resorptive process, in both the short and long term, will lead to bone deficit or dentoalveolar deficit, which needs to be corrected and restored before any rehabilitation strategy is undertaken and executed. If a patient is willing to have a bridge, this bone resorption causes gaps, food impaction, aesthetic compromise, and functional deficit. The same applies to the provision of an implant-supported single crown, whereby there is insufficient bone for safe implant placement, retention, stability, and successful rehabilitation.
The alveolar ridge may need to be restored to ensure long-lasting and stable tooth replacement utilising dental implants.
Why Socket Preservation is Critical?
The function and aesthetics of implant-supported teeth can be severely compromised when supporting bone and gum are deficient. Replacing lost tooth with implant-supported crown option is impossible in absence of intact bone.
In absence of bone augmentation, bone defects due to trauma or extracted teeth or gum recession may develop around neck of implant, resulting in aesthetic and biological complications, especially in aesthetic zone.
Although bone grafting procedure is often very successful, some biological complications such as infection or resorption may interfere with successful graft integration and consolidation.
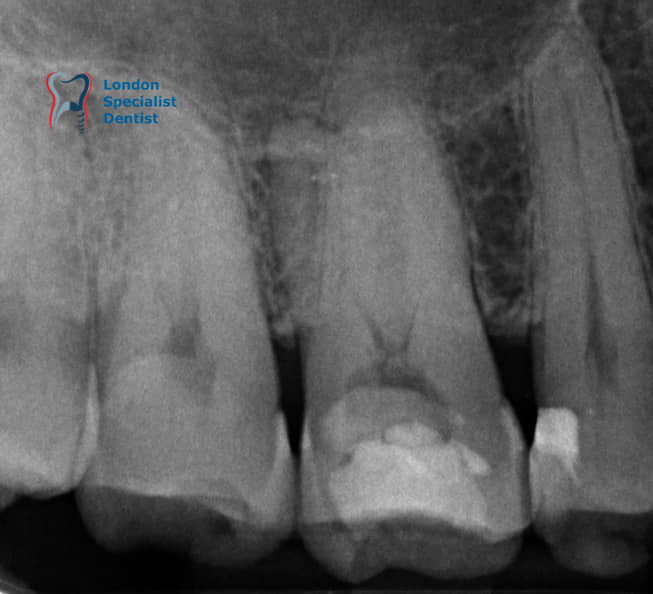
Before extraction
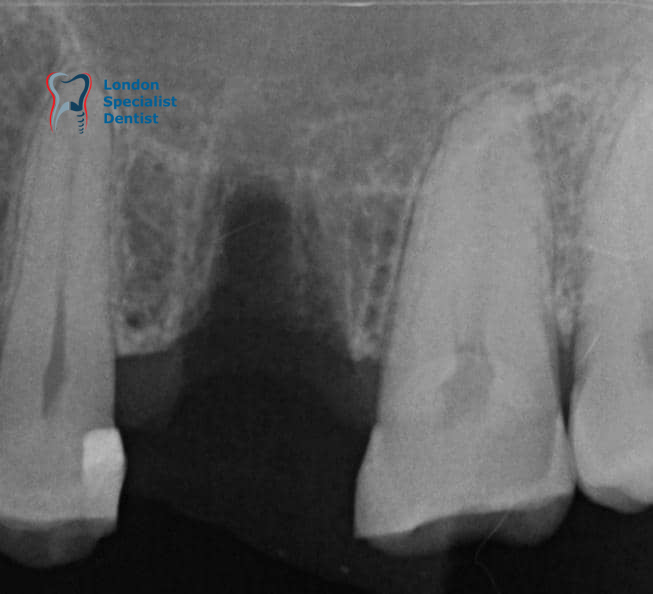
After extraction
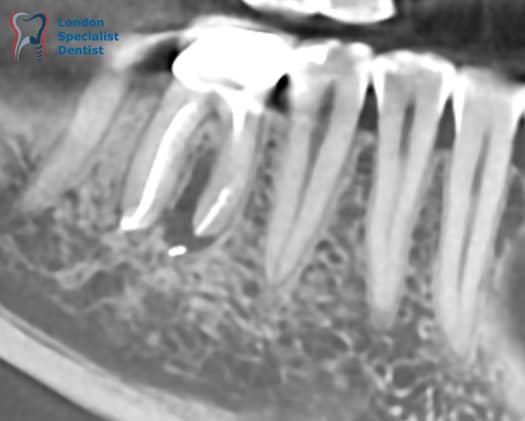
Sagittal aspect of the CBCT from infected tooth

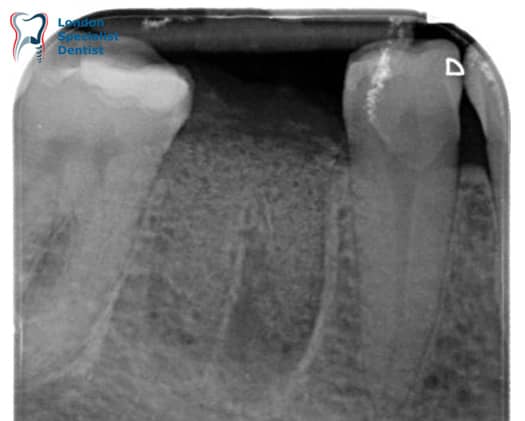
After extraction
Ridge Preservation
What Happens to Alveolar Ridge After Tooth Extraction?
Based on evidenced-based clinical and histological studies, preservation of alveolar bone architecture depends on both physiologic and mechanical stimulation maintenance of tooth in alveolar socket. Rate of dimensional changes in extraction site could be more rapid during post-extraction immediate 2-3 months periods, while more gradual after that.
Existence and resorption rate of bundle bone which forms walls of tooth socket are dependent on blood supply from periodontal ligament, which disintegrates after tooth extraction. Horizontal bone loss progresses more extensively in buccal-lingual direction.
Factors Determining Resorption Rate
Following tooth extraction, resorptive bone changes take place around extraction site. Extent of post-extraction bone loss influenced by:
- The traumatic nature of root elevation and type of flap raised during surgery (split thickness versus full thickness)
- Systemic and local biological health of patient
- Patient’s lifestyle, such as smoking
- Number of roots
- Pre-extraction dimensions of peripheral alveolar bone
- Hard and soft tissue biotype
How Bone Resorption Progresses
According to scientific evidence:
About 50% of alveolar socket bone ridge width resorption occurs during first year, with highest resorption rate during immediate post-extraction period by average of 1mm within first three months.
Bone resorption occurs more extensively horizontally around buccal bundle bone and around anterior teeth as buccal bone plate is thinner than lingual side.
What Is Atraumatic Tooth Extraction?
Surgical trauma caused by tooth extraction can be limited by using minimally invasive approach, which reduces risk of micro-fractures in thin surrounding socket housing and decreases resorption rate. Atraumatic tooth extraction performed to minimise mechanical, chemical, bacterial, or biological trauma to socket walls.
How Do We Perform Atraumatic Extraction?
The process includes:
- Detailed clinical evaluation of anatomical features near planned extraction site
- Assessing anatomical landmarks around tooth subject to extraction
- Loosening and segmenting roots when tooth is endodontically treated, to reduce undue mechanical trauma to alveolar socket
- Careful removal of periodontal ligament, excavation of infected tissues
- Possible use of L-PRF and Ridge preservation when indicated
What Is Ridge Preservation?
In absence of bone augmentation, ongoing bone resorption around neck of implant causes aesthetic and biological complications, especially in aesthetic zone. Use of Bone replacement materials (BRMs) minimises extent of bone resorption.
Ridge preservation prevents ongoing bone loss after tooth extraction by maintaining socket height and width, preserving bone architecture for future implant placement.
How Do We Perform 3-Dimensional Socket Preservation?
After thorough socket debridement, socket will be filled by bone grafting using Bone Replacement Materials (BRM). Augmented socket should be sealed with biological barrier which prevents displacement or early resorption of graft material. In end, socket will be covered using pedicle gum grafts.
Clinical Process of Socket Preservation:
Stage 1: Assessment
- Clinical evaluation and imaging
- Radiographic assessment
- Treatment planning
Stage 2: Atraumatic Extraction
- Minimally invasive extraction technique
- Socket debridement and preparation
- L-PRF collection if indicated
Stage 3: Graft Placement
- Place bone replacement material in socket
- Apply collagen or e-PTFE membrane barrier
- Seal extraction site
Stage 4: Healing and Preservation
- Guided bone regeneration occurs
- Socket height and width maintained
- Bone consolidation and remodelling (1-6 months)
Stage 5: Implant Placement
- Place dental implant in preserved socket
- Adequate bone height and width available
- Optimal implant positioning achieved
Bone Replacement Materials For Socket Preservation
AUTOGRAFTS
Human autogenous bone grafts harvested from upper or lower arches such as wisdom tooth or chin. Autogenous bone can also be collected during implant drilling procedures.
ALLOGRAFTS
Human bone grafts harvested from other human beings and processed from bone banks. All allografts processed from donors found negative by FDA-approved tests for HBsAg, anti-HBc, anti-HCV, and STS. Anti-HIV and anti-HTLV-I. Although efforts made to ensure quality, most tissue banks make no claims concerning biological or biomechanical properties of provided allograft.
XENOGRAFTS
Bio-Oss is natural bone mineral derived from bovine (cow) bone with similar micro-architecture to human bone. Bio-Oss promotes bone scaffolding and has osteoconductive properties promoting ingrowth of blood vessels and bone cells which gradually integrate into native bone completely. Bio-Oss particles may remain in tissue bed surrounded by native natural bone.
ALLOPLASTS
Bone ceramic particulates such as Maxresorb or Regen are synthetic bone graft materials made from biphasic tri-calcium phosphate naturally present in our bone. Based on micro-porosity of particulated grafts, resorption profile varies from three to twenty months.
BIOLOGICAL MEMBRANES
Protective membranes could be non-resorbable (e-PTFE) or collagen membrane derived from porcine (pig) or bovine (cow) collagen. Membrane protects graft particulates within scaffold of bone defect periphery while preventing displacement and early resorption of graft material. Most collagen membranes resorb entirely by body following bone regeneration.
Important note: If you do not wish to consent to have any animal-derived graft or membrane products, please inform your doctor before signing consent forms.
Socket Preservation – Clinical Application
Socket preservation procedure may be performed by specialist periodontist using various techniques and materials including synthetic products, animal/human derived biomaterials. Based on amount of bone required and patient’s preference, one or mixture of bone replacement materials may be used.
Our experienced surgeons in London Specialist Dentists apply most scientifically approved material and techniques in field of socket preservation throughout surgical procedures to improve long-term biological success and ensure optimal bone volume for future implant placement.
Clinical Expertise:
Dr. Kamosi specialises in advanced bone regeneration, guided bone regeneration (GBR), ridge preservation, socket preservation, sinus augmentation, and atraumatic tooth extraction. Expertise in surgical implantology and restorative prosthodontics enables him to deliver predictable outcomes in complex cases requiring bone augmentation and implant-supported restorations. Particularly skilled in full-mouth rehabilitation and aesthetic dentistry, combining biological principles with advanced surgical technique.