
What is gum recession?
Gum recession, also known as receding gum could be defined as the clinical loss of gum margins toward and along the root surface. Gingival recession or gum recession could be caused by the damage to the tooth-supporting periodontal tissues, i.e. fibres, cementum, and alveolar bone, such as iatrogenic factors, orthodontic movement, chemical trauma, e.g. chewing betel nuts, and infectious oral disease.
Periodontal disease, aggressive oral hygiene activities, frenal pull, bone dehiscence, defective restorations, tooth misalignment, viral and bacterial infections have all individually or in combination been associated with the gum recession. The clinical signs and symptoms attributed to gum recession are tooth dentin hypersensitivity, root caries, and disturbing aesthetic.

Mucogingival deformities:
The presence of marginal tissue recession is associated with:
1. Traumatic toothbrushing (Khocht et al. 1993), Para-functional activities/p>
2. Alveolar bone dehiscences (Bernimoulin & Curilivic 1977; Løst 1984),
3. High muscle attachment and frenal pull (Trott & Love 1966),
4. Plaque and calculus (van Palenstein, Helderman et al. 1998; Susin et al. 2004),
5. Iatrogenic factors related to traumatic restorative and periodontal treatment procedures (Lindhe & Nyman 1980; Valderhaug 1980),
6. Periodontal CAL loss may cause compensatory remodelling and MBL, hence apical migration of gingival margin (Serino et al. 1994).
7. Inter-dental attachment/bone loss, NUG, NUP
8. Inadequate zone of attached gingival may be addressed to withstand the traumatic mechanical, iatrogenic restorative, surgical, and orthodontic procedures. With respect to orthodontic therapy, this would imply that as long as a tooth is moved exclusively within the alveolar bony housing, soft tissue recession will not develop (Wennstrøm et al. 1987).
9. Localised dental restorative prosthesis-related factors
Addressing the contributory Factors:
1. High aberrant muscle & frenal attachment
Frenectomy & dissection of fibre pull; Follow- up to see the outcome of the frenectomy in the form of frenal relapse and rebound due to high muscle pull and short vestibulum
2. Localised prosthesis-related factors:
Eliminate the non-biologically compatible elements by prosthetic modification
3. Reduced vestibular depth
Increase the vestibular depth (e.g. denudation plus FGG):
4. Inadequate zone of attached gingival:
Increase the width & thickness of the keratinized attached gingiva to prevent a further recession?
5. Dentin hypersensitivity:
Achieve root coverage at the affected tooth to alleviate root hyper-sensitivity
The most efficient clinical approach to the restoration of the gum recession defects both in the short- and long-term is the implementation of periodontal plastic surgery or gingival transplant surgery.
The specialists in LSD will offer you the most well-documented treatment strategies available. These techniques include free gingival, gum tunnelling techniques, and connective tissue transplant alone or combined with guided-tissue-regeneration (GTR) strategies.
Management of the mucogingival deformities
1. CAUSE-RELATED THERAPEUTIC SCHEDULE, TREATMENT:
Traumatising tooth brushing technique & para-functional activities
- Information about the aetiology and treatment strategies of gum recession.
- Oral hygiene instruction.
- Modification of brushing technique with a soft brush.
2. CORRECTIVE/ REHABILITATION PHASE OF THERAPY (MUCO-GINGIVAL/ PERIODONTAL PLASTIC SURGERY):
Conventional Gingival Transplant
Gum Recession After Wearing Braces Can Now Be Treated Without Gum Grafting Surgery.
GTR is the latest sophisticated surgical technique thatrestores the hard tooth-supporting tissues itoenhance the long-term prognosis of your tooth. GTR combined with periodontal plastic surgery are the procedures by which the deficits in compromised architecture and function of the periodontal tissues are restored.
Clinical application of gingival plastic surgery
Gum recession on the tooth 31 (LL1) cervical margin

Root coverage following the surgical gum transplant
Tunnelling Gum Regeneration
Most periodontal specialist or soft tissue plastic surgical protocols involve the correction of gum or mucogingival deficiencies and root coverage. Albeit, there is a need to optimise the currently implemented conventional treatment strategies to diminish the untoward postoperative surgical morbidity or discomfort, and optimise their clinical outcome.
The currently advocated minimally invasive surgical protocols have addressed some of the concerns for potential surgical trauma when regenerating the soft-tissue deficiencies and root exposure.
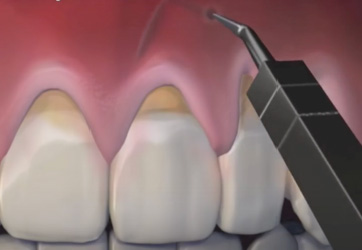
The modified Vestibular Incision Supra-periosteal Tunnel Access (M-VISTA) has been claimed to implement the principles of minimally invasive mucogingival surgery to optimise the treatment outcome and patient-reported outcome measurements (PROMs).
The recently well-published minimally invasive (M-VISTA) involve supra-periosteal key-hole access, tunnelling tissue bed preparation, and soft tissue graft stabilisation.
The M-VISTA technique is claimed to reduce surgical time and increase patient comfort by preventing trauma to the periosteum and reducing the grafted connective tissue vascularity.
A tension-free coronally advanced supra-periosteal mucosal flap will preserve the structural and vascular integration of the papilla. as opposed to the non-autogenous graft, the connective tissue may enhance the zone of keratinization. In such procedures, graft stabilization is crucial for increased plasmatic perfusion and vascular circulation.

Miller Class II / Cairo RT1
Miller Class II / Cairo RT1

Incision and release of the mucoperiosteal flap
Tunnelling and release of the mucosal flap

Flap elevation and CTG in-Situ

Tunnelling and coronal advanced flap

External suturing of advanced flap and CTG

Internal stabilisation of advanced flap and CTG