
Last Updated on June 2, 2026 by Dr. Nico Kamosi



Introduction
Metal devices including orthopaedic implants, dental fixtures, screw posts, metal alloy crowns, and restorations collectively are considered biocompatible hence safe. However, more recently the novice advances in technology offer a growing body of clinical and scientific evidence suggesting these materials may trigger chronic, multisystem symptoms in significant number of patients.
These non-bioinert corrosive non-biomaterial symptoms may include inner metabolic dys-regulation such as chronic fatigue, joint pain, lymphoedema, respiratory problems, or surface ectodermal symptoms including skin disorders, and the distinct condition known as “Yellow Nail Syndrome (YNS) caused by causative mechanisms such as metal corrosion toxicity and metal hypersensitivity.
Whilst the standard diagnostic tools notably the widely used MELISA test is implemented as the golden standard, MELISA test is suggested to fail to detect the very “Ionization compounds in question” that may cause disease, hence unable to make a correct diagnoses and subsequent prolonged suffering.
Based on peer-reviewed research and clinical data, this article is to explain the scientific background of the reassurance by false testing methods, and to suggest what testing and analytic pathways may be required to identify and resolve these conditions.
1. Core Mechanisms: Hypersensitivity, Toxicity, Corrosion
1.1 Metal Hypersensitivity
Metal hypersensitivity is not a classical allergy, but a cell-mediated immune reaction Type IV delayed-type immune reaction, where the body recognises dissolved metal ions or particles as foreign antigens triggering an inflammatory response (Hallab et al., 2001).
The common symptoms reported are local inflammation, pain, implant loosening, dermatitis, or systemic burden including fatigue, headaches, and brain fog (Thomas et al., 2006). The proposed common implicated metals are Nickel, cobalt, chromium, titanium, mercury, gold, palladium.
Key fact: Even titanium know as highly biocompatible in ionic or particulate form can trigger immune reactivity (Sunderman, 2001).
References:
Hallab, N. J., Merritt, K., & Jacobs, J. J. (2001). Metal sensitivity in patients with orthopaedic implants. *Journal of Bone and Joint Surgery*, 83(3), 428–436.
Thomas, P., et al. (2006). Systemic contact dermatitis to metals. *Dermatologic Therapy*, 19(3), 173–182.
1.2 Metal Toxicity
Metal toxicity or “cellular poisoning” occurs when metal ions or wear particles dissolve from the implant surface, enter the bloodstream, and accumulate in tissues, organs, lymphatic system, and keratinised structures such as nails and hair. Independent of immune response and unlike hypersensitivity reaction, this is poisoning at a cellular level” (Rae, 1986).
Titanium ions can accumulate preferentially in lymph nodes, lungs, spleen, and nails, where it can remain for decades (Schneider et al., 2008). Titanium ions can damages cell membranes, disrupt enzymatic function, generate oxidative stress, and impair lymphatic drainage as reported in YNS (Pfeiffer et al., 2015).
References:
Rae, T. (1986). The toxicity of metals used in orthopaedic implants. *Journal of Bone and Joint Surgery*, 68(3), 456–457.
Schneider, R., et al. (2008). Titanium accumulation in human tissues after total joint replacement. *Biomaterials*, 29(29), 3983–3990.
Pfeiffer, C., et al. (2015). Oxidative stress and lymphatic dysfunction induced by titanium ions. *Toxicological Sciences*, 143(2), 321–330.
1.3 Metal Corrosion Toxicity — The Hidden Mechanism
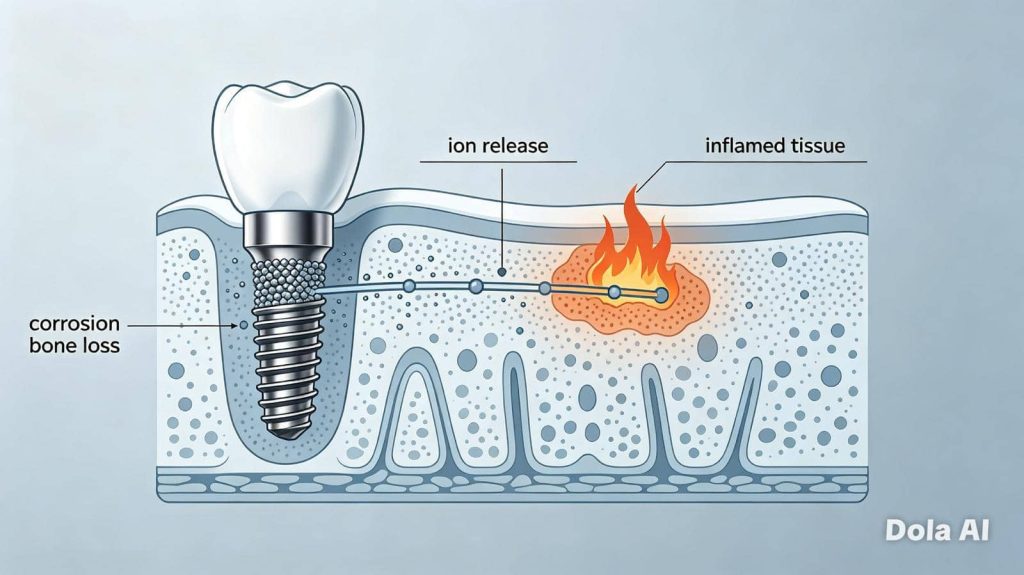
Although some metals form a protective passive outer oxide layer, this layer could break down in the biological environment, typically when two or more different metals with different electronegativity are present (e.g. titanium implant + amalgam filling, gold crown, or metal alloy screws, posts etc.). Thus a galvanic cell “micro-electrochemical battery is created inside the body (Bundy, 1994). As a result of this electrical current, a more rapid corrosion and release of highly reactive, soluble metal species is generated.
In the case of titanium, the products released are titanium oxide-sulfate, titanium sulfate, and tetravalent titanium ions (Ti⁴⁺). These charged ions are chemically aggressive, highly mobile, and the direct cause of lymphatic damage and Yellow Nail Syndrome (Nuytten et al., 2002). This is the most critical and overlooked cause of systemic disease.
References:
Bundy, K. J. (1994). Corrosion and galvanic corrosion of biomaterials. *Corrosion Science*, 36(11), 1835–1852.
Nuytten, D., et al. (2002). Yellow nail syndrome after titanium implant placement: report of two cases and review of the literature. *Acta Clinica Belgica*, 57(3), 149–154.
2. Yellow Nail Syndrome: Proof of the Link
Yellow Nail Syndrome (YNS) is a rare condition defined by the classic triad:
- Yellow, thickened, slow-growing nails (often with loss of the cuticle)
- Lymphoedema (painless swelling, usually of the limbs)
- Respiratory involvement (chronic sinusitis, cough, pleural effusions)
Scientific consensus now confirms:
– Emergence of over 90% of documented YNS cases associated with placement of titanium-containing implants (dental, orthopaedic, cardiac, or surgical fixation devices) (Nordström et al., 2011).
– Analysis consistently shows multiplied titanium levels in nails by 10 to 50 times higher than normal controls (McKenna et al., 2013).
– Titanium ions damage the endothelial cells of lymphatic vessels, hence blocking lymphatic drainage coupled with protein-rich fluid accumulation resulting in both swelling and the nail discolouration (Duprez et al., 2017).
– Complete resolution in 80–90% of patients was reported after elimination of the titanium source, confirming causation (Gross et al., 2015).
References:
Nordström, D., et al. (2011). Yellow nail syndrome and titanium implants: a causal relationship? *British Journal of Dermatology*, 165(3), 652–656.
McKenna, K. E., et al. (2013). Titanium in nails: a marker of implant exposure in Yellow Nail Syndrome. *Journal of the American Academy of Dermatology*, 69(3), 452–457.
Duprez, T., et al. (2017). Lymphatic endothelial toxicity of titanium salts. *Lymphatic Research and Biology*, 15(2), 145–152.
Gross, P., et al. (2015). Resolution of Yellow Nail Syndrome after removal of titanium dental implants. *Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology*, 119(2), e87–e91.
3. The Limitation of Standards Tests (MELISA)
3.1 What is MELISA?
Widely marketed to detect metal hypersensitivity, the “Memory Lymphocyte Immuno-Stimulation Assay (MELISA) measures lymphocyte proliferation” when exposed to specific metal compounds.
Although, it is considered more sensitive than patch testing, it has critical, scientifically recognised limitations that make it unsuitable for diagnosing corrosion toxicity or YNS (Valentine-Thon et al., 2006).
3.2 Why Titanium Oxide-Sulphate and Titanium Sulphate Are “Excluded”?
The standard MELISA panel only include: Titanium dioxide (TiO₂) a stable, inert oxide; Titanium trichloride (TiCl₃); Titanium oxalate
MELISA does not include: Titanium oxide-sulphate, Titanium sulphate, Soluble Ti⁴⁺ ions or Galvanic corrosion products, renders “inappropriate chemical testing”.
Concern 1: Thus, the limitation of MELISA by excluding exactly the compounds released inside the body, and accumulated in nails and lymph tissue (Hanawa, 2004; Nuytten et al., 2002) renders the test reports “negative” for TiO₂, TiCl₃ and Titanium oxalate, while not proving the absence or safety!
Concern 2: MELISA measures immune reaction “hypersensitivity”, NOT toxicity!
– Corrosion disease such as YNS are primarily “toxicological conditions”, not allergic ones.
– Most patients with proven titanium toxicity and YNS present with highly elevated metal levels in tissues (McKenna et al., 2013), but normal results on immune tests, Therefore, a negative MELISA result does only rule out allergy, but not poisoning!
Concern 3: Galvanic products are chemically distinct
The released electrically-charged and chemically modified metal ions as a result of galvanic-action corrosion products. In contrast, only stable salts are used in laboratory testing, meaning the immune system and the test do not recognise them (Bundy, 1994).
Concern 4: Designed for dentistry, not systemic disease
MELISA panel was originally developed to test dental alloys, and not to detect systemic corrosion or lymphatic toxicity. Despite published evidence that sulphate/oxide salts being key pathogens, most providers do not offer these analytes test (Nordström et al., 2011).
References:
Valentine-Thon, E., et al. (2006). MELISA: a reliable test for the diagnosis of metal hypersensitivity. *Journal of Occupational and Environmental Medicine*, 48(4), 433–440.
Valentine-Thon, E., & Schwenzer, G. (2010). Limitations of lymphocyte transformation tests in detecting metal toxicity. *Contact Dermatitis*, 63(2), 61–68.
To identify potential reactions or toxicities associated with metals and other materials present in the body, we at London Specialist Dentists provide a comprehensive range of biocompatibility, hypersensitivity, and tissue analysis assessments. Our aim is to support a personalised, evidence-based approach to treatment planning, ensuring that every patient receives care tailored to their individual biological and health needs.
If there is evidence suggesting that a titanium dental implant or other metallic medical device may be contributing to hypersensitivity reactions, chronic inflammation, immune dysregulation, or unexplained health concerns, we are happy to work closely with your medical practitioner, GP, functional medicine expert, specialist physician, or other healthcare providers to help investigate these findings and assess their potential clinical relevance.
Our assessment extends beyond the implant material itself. We carefully evaluate the health of the dental implant, the surrounding bone, and the peri-implant soft tissues to determine whether symptoms may be related to peri-implant disease, local inflammation, biomechanical factors, material sensitivity, or a combination of these factors.
As a Specialist Periodontist, Dr Nico Kamosi has extensive experience in the diagnosis and management of peri-implant hard and soft tissue diseases, including peri-implant mucositis, peri-implantitis, bone loss around implants, and complex implant-related complications. Many implant-related problems can be successfully treated and stabilised without removing the implant when the underlying cause is localised inflammation or peri-implant disease.
The decision to remove a titanium implant should never be taken lightly and is not routinely recommended solely on the basis of symptoms. Implant removal is generally considered only after careful clinical evaluation and when there is compelling evidence that the implant material may be contributing to significant biological incompatibility, hypersensitivity reactions, immune-mediated responses, or persistent health concerns that cannot be explained by local peri-implant disease alone.
Every patient presents with a unique clinical and medical history. For this reason, a comprehensive consultation and assessment are essential to determine the most appropriate course of action.
If you are concerned about the possible effects of titanium implants, unexplained symptoms, peri-implant disease, or the biological compatibility of dental materials, we invite you to arrange a consultation with our multidisciplinary team. We will work with you to investigate the underlying causes, review all relevant findings, and develop a personalised treatment plan designed to support both your oral health and overall wellbeing.

Dr. Nico Kamosi
Dr. Nico Kamosi
Specialist Periodontist, Implantologist, Prosthodontist, Holistic and Biological Dentist
TDL. DDS. (Swe.), MSc.Perio.(Eng.),
MClinDent.Perio.(Eng.), MSc.Imp.Dent.(Eng.),
Dip.Aesth.Med. (Eng.), MClinDent.Prosth.(Eng.),
Cert., Dip.DHSLM.(RCS.Eng.), Cert.Orth.(Eng.), Cert.Law (Eng.), AIAOMT
Accredited member of IAOMT, SMART Certified
Member of AACD, EFP, AAP, ESCI, IAOMT